Anatomy
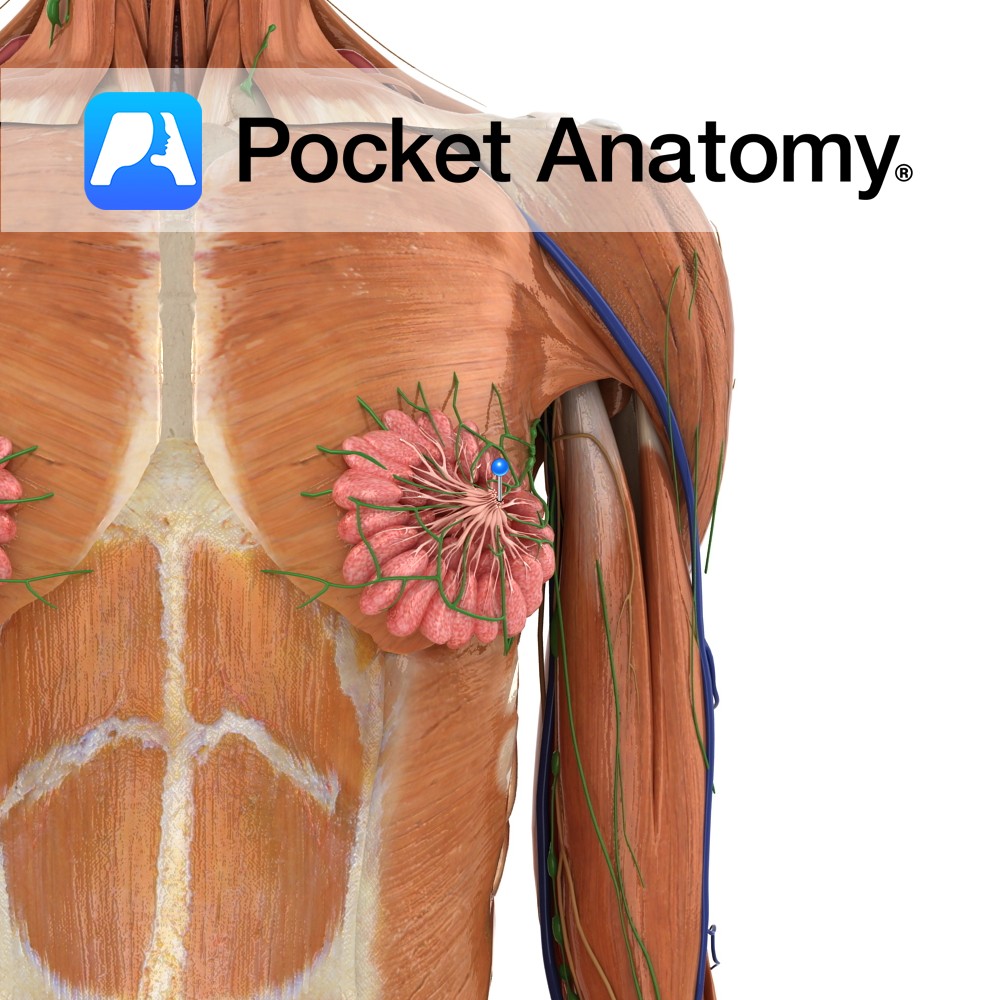
(nipple/papilla/teat) Small (about 1cm, size varies, bigger during and subsequent to lactation) skin-covered projection/bump/eminence on front centre of breast (surrounded by sensitive pigmented areola with Montgomery’s tubercles), onto the surface of which project the ends/openings of 5-20 milk ducts from related breast lobules and their acini. Pigmented brown (also areola, more so after pregnancy), rich in nerve endings. Innervated by 4th inter-costal nerve.
Physiology
Erection/swelling of nipple (male/female) caused by (circular and radiating areolar) smooth muscle contraction (as with “goose bumps” and hair “standing on end”); caused by heat/arousal; oxytocin stimulates in breastfeeding. Babies have rooting/suckling instinct by which they latch on to nipple, forming a suction-seal, the resulting breastfeeding pleasurable to mother/child and contributing to bonding. An erogenous zone (stimulation can sexually arouse) generally stimulated by hand/mouth. Supernumerary, usually non-functional nipples common.
Clinical
Cracked nipples; painful condition particularly if breastfeeding, causes include over-washing/drying or prolonged wetting – interruption of function of Montgomery’s glands which ordinarily secrete appropriate lubricant/film; also traumatic irritation (sa repetitive rubbing in athletic activities), eczema, Paget’s disease (cancer originating in ducts/lobules). Accessory/supernumerary nipple common (1% m/f), usually along a line from axilla to groin (embryonic milk line). Gynecomastia (prominent nipples and breasts in men) common; physiologic (temporary male/female hormone imbalance during growth phase) and resolving in babies, puberty; can persist into adulthood and lead to surgical treatment. Needs to be distinguished from male breast cancer (1% of all breast cancer).
Interested in taking our award-winning Pocket Anatomy app for a test drive?
![]()