Anatomy
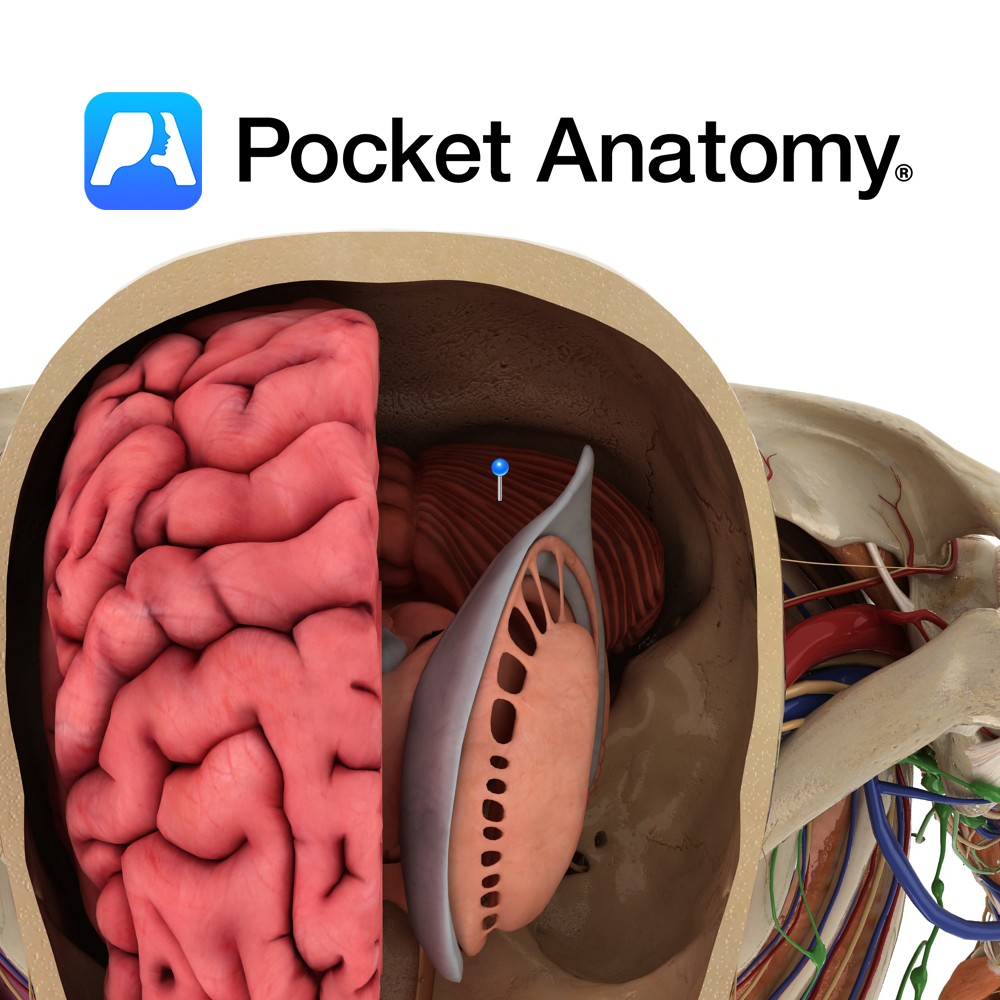
Located in the posterior cranial fossa, inferior to the cerebrum and posterior to the pons and medulla and forms the roof of the 4th ventricle. Composed of two cerebellar hemispheres, connected by the midline vermis. The dural tentorium cerebelli separates the cerebellum below from the occipital lobes above, while the dural falx cerebelli intervenes between the cerebellar hemispheres.
The cerebellum is divided anatomically into three lobes: an uppermost anterior lobe separated from the posterior lobe beneath by the primary fissure and the flocculonodular lobe separated from the posterior lobe above and behind by the posterior fissure.
Functionally the cerebellum is also divided into three lobes, the archicerebellum (vestibulocerebellum), paleocerebellum (spinocerebellum) and neocerebellum (cerebrocerebellum). All of the inputs and outputs to the cerebellum pass through the inferior, middle, or superior cerebellar peduncles (ICP, MCP, SCP respectively)
Blood Supply:
Three pairs if vessels supply the cerebellum, namely the anterior inferior, posterior inferior and superior cerebellar arteries (AICA, PICA SCA).
Functions
Motor coordination involving balance, posture and muscle tone.
Clinical
Lesions of the cerebellum can result in a variety of clinical syndromes depending on the site of the lesion. Cerebellar dysfunction may result in disturbance of motor control (including of limb, pharyngeal and oculomotor), skilled movement coordination, and hypotonia. Specific manifestations of cerebellar dysfunction include ataxia, dysarthria, tremor, and nystagmus. Clinical syndromes relating to the cerebellum may be divided into those affecting the vermis, a cerebellar hemisphere, or may be pancerebellar.
Cerebellar vermis lesions are characterised by axial dysequilibrium, broad-based ataxic gait, with minimal or no appendicular (limb) ataxia, and occasionally presence of spontaneous nystagmus (if caudal vermis involved). Chronic alcohol toxicity commonly displays localised pathology to the rostral vermis. Medulloblatomas may preferentially involve the caudal vermis.
Cerebellar hemisphere lesions are are characterised by appendicular incoordination (including limb past pointing and intention tremor, impaired fine finger movements, dysdiadochokinesia) on the ipsilateral side, and dysarthria. Common aetiologies are space occupying lesions (e.g. neoplasm, abscess) and infarcts.
Pancerebellar syndrome combines features of bilateral cerebellar hemispheres and cerebellar vermis. Common aetiologies include paraneoplastic disorders, infectious and parainfectious causes, and toxic-metabolic disorders.
Interested in taking our award-winning Pocket Anatomy app for a test drive?
![]()