Anatomy
Origin:
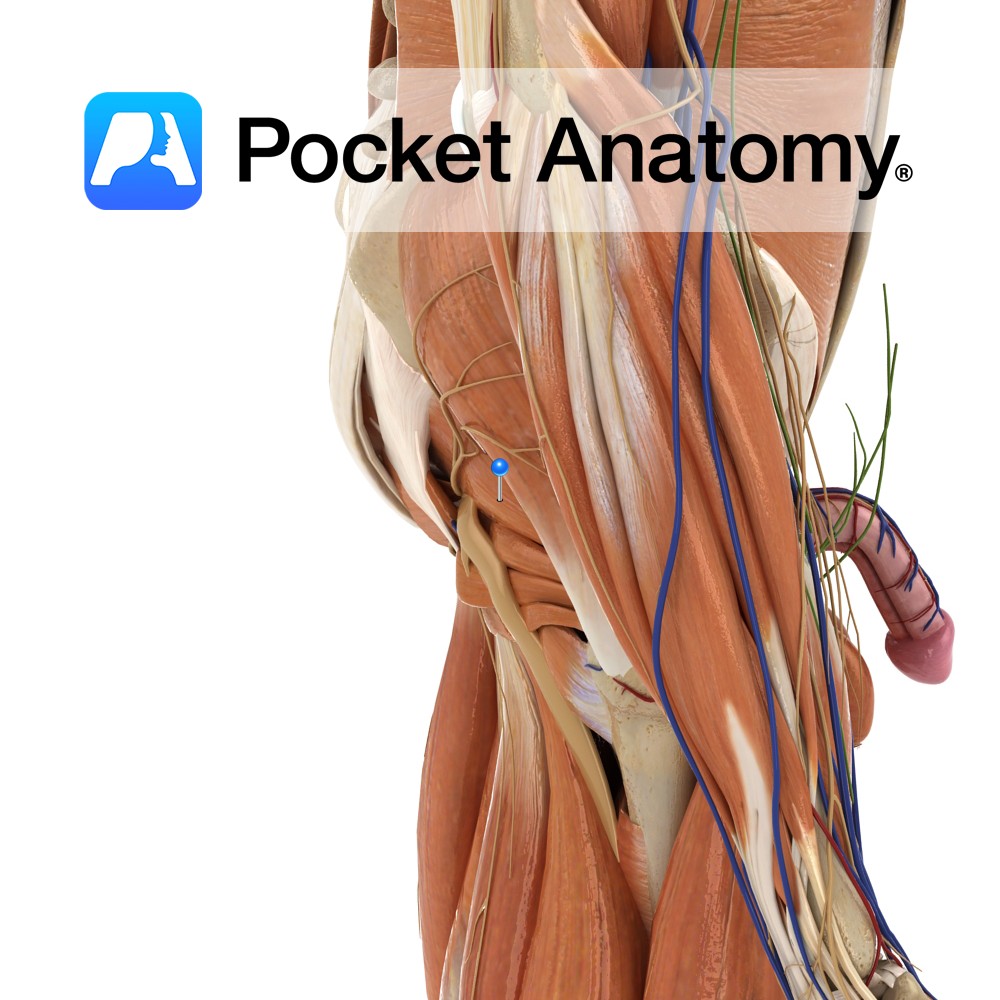
Anteriolateral surface of the sacrum by three digitations, greater sciatic notch and sacrotuberous ligament.
Insertion:
After passing through the greater sciatic foramen, inserts into medial side on the superior border of the greater trochanter of the femur.
Key Relations:
-Divides the greater sciatic foramen. Only the superior gluteal nerve passes superior to it. All other nerves normally pass inferior.
-Therefore the sciatic nerve normally exits the pelvis below the piriformis. However the sciatic nerve passes through the piriformis muscle in approximately 15% of the population predisposing them to piriformis syndrome (See clinical for more information).
Functions
-Laterally rotates the extended thigh at the hip joint.
-Abducts the flexed thigh at the hip joint.
Supply
Nerve Supply:
Nerve to piriformis (S1, S2).
Blood Supply:
-Branches of the internal iliac arteries including the superior and inferior gluteal arteries
-Lateral sacral arteries.
Clinical
Piriformis syndrome is compression of the sciatic nerve by the piriformis muscle. It causes pain in the buttocks and referred pain along the sciatic nerve. This referred pain is known as sciatica. Sitting down, hip flexion and internal rotation increases pain. Exacerbation of pain on internal rotation is known as Pace’s sign.
Treatment is variable and involves rest, ice, stretching, physical treatment and oral or injectable anti-inflammatory drugs including corticosteroids.
Interested in taking our award-winning Pocket Anatomy app for a test drive?
![]()