Anatomy
Origin:
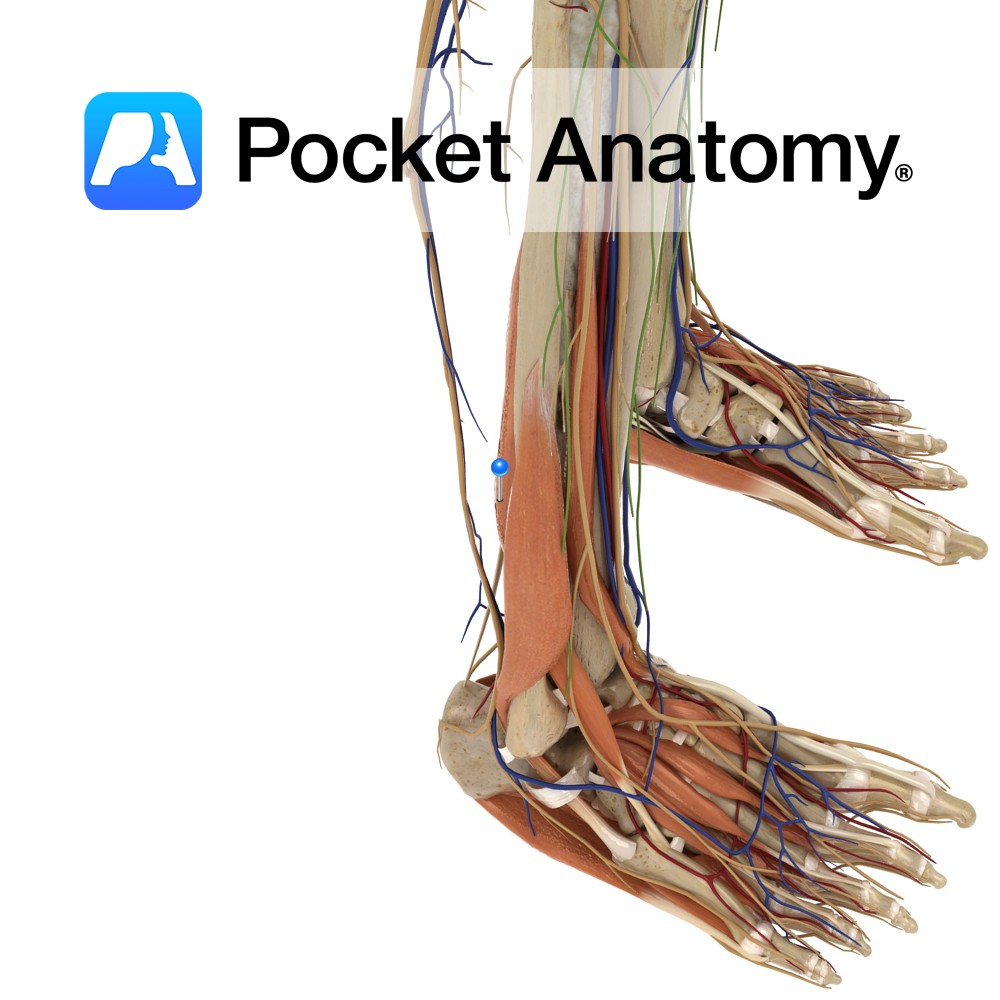
Lower two-thirds of the posterior surface of the fibula, the posterior intermuscular septum and the posterior surface of the distal part of the interosseous membrane.
Insertion:
Plantar surface of the base of the distal phalanx of the hallux (big toe).
Key relations:
-One of the four muscles of the deep posterior compartment of the leg.
-The flexor hallucis longus tendon passes posterior to the flexor digitorum longus tendon.
Functions
-Flexes the hallux (big toe).
-Weakly plantarflexes the ankle joint.
-It acts during final propulsion in gait e.g. pushing off the surface in walking.
-Assists in the maintenance of the medial longitudinal arch.
Supply
Nerve Supply:
Tibial nerve (L5, S1, S2).
Blood Supply:
–Posterior tibial artery
-Fibular (peroneal) artery.
Clinical
Flexor tendinitis is inflammation of the flexor tendons of the toes such as flexor digitorum longus and flexor hallucis longus. It is most commonly seen in sports injuries and dancers. Flexor tendinitis although often more painful is not as common as extensor tendinitis. The patient may present with pain and swelling along the course of the tendons, arch of the foot and postero-medial ankle with pain and weakness on push-off as well as increased pain with resisted flexion of the hallux (big toe). Large quantities of synovial fluid may be present within the tendon sheath on MRI.
Treatment includes rest, ice, NSAIDs and taping of the foot to support the arch. More severe cases may require surgery which has proven very successful with a recovery period of approximately 6 to 9 weeks.
Interested in taking our award-winning Pocket Anatomy app for a test drive?
![]()