PocketAnatomy® is a registered brand name owned by © eMedia Interactive Ltd, 2009-2022.
iPhone, iPad, iPad Pro and Mac are trademarks of Apple Inc., registered in the U.S. and other countries. App Store is a service mark of Apple Inc.
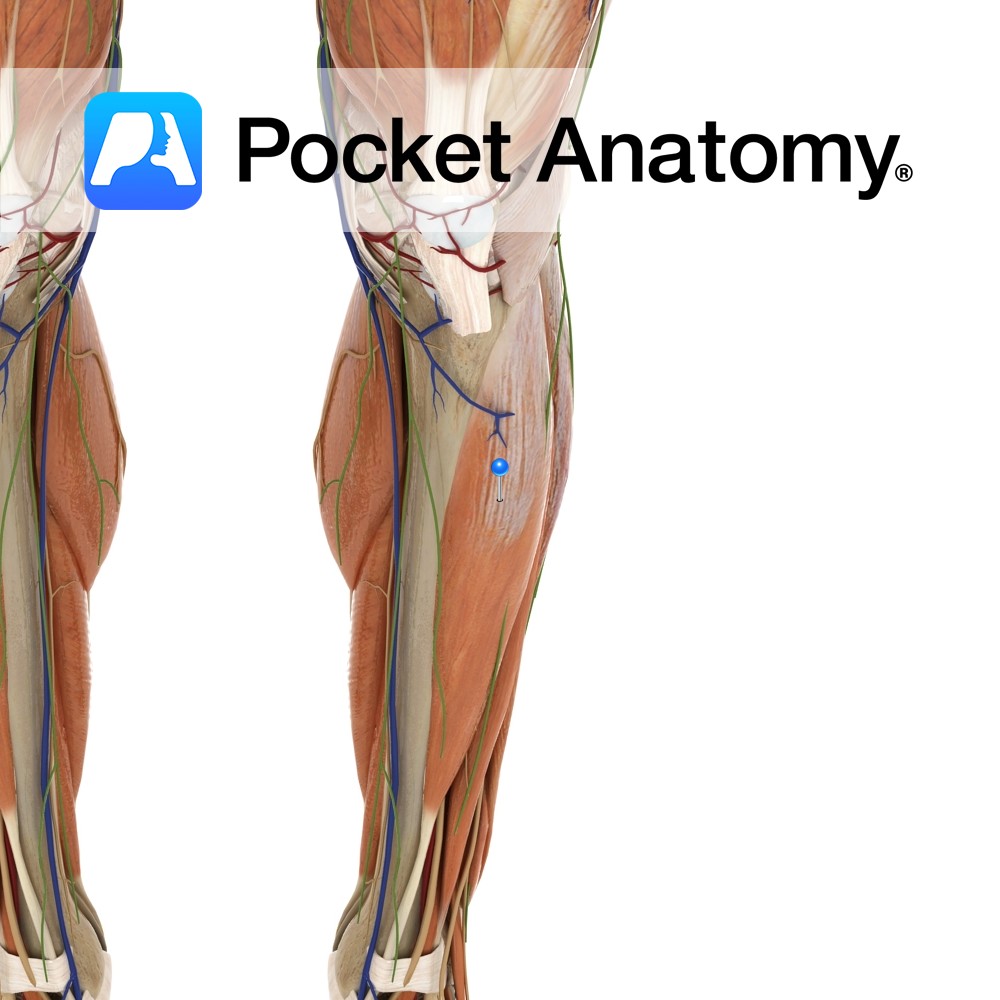
Anatomy Origin: Inferior surface of the lateral condyle and upper two-thirds of lateral surface of the tibia and the interosseous membrane. Insertion: Medial surface of the medial cuneiform and the base of 1st metatarsal. Key Relations: -One of the four muscles of the anterior compartment of the leg. -The tibialis anterior tendon crosses anterior to
- Published in Pocket Anatomy Pins
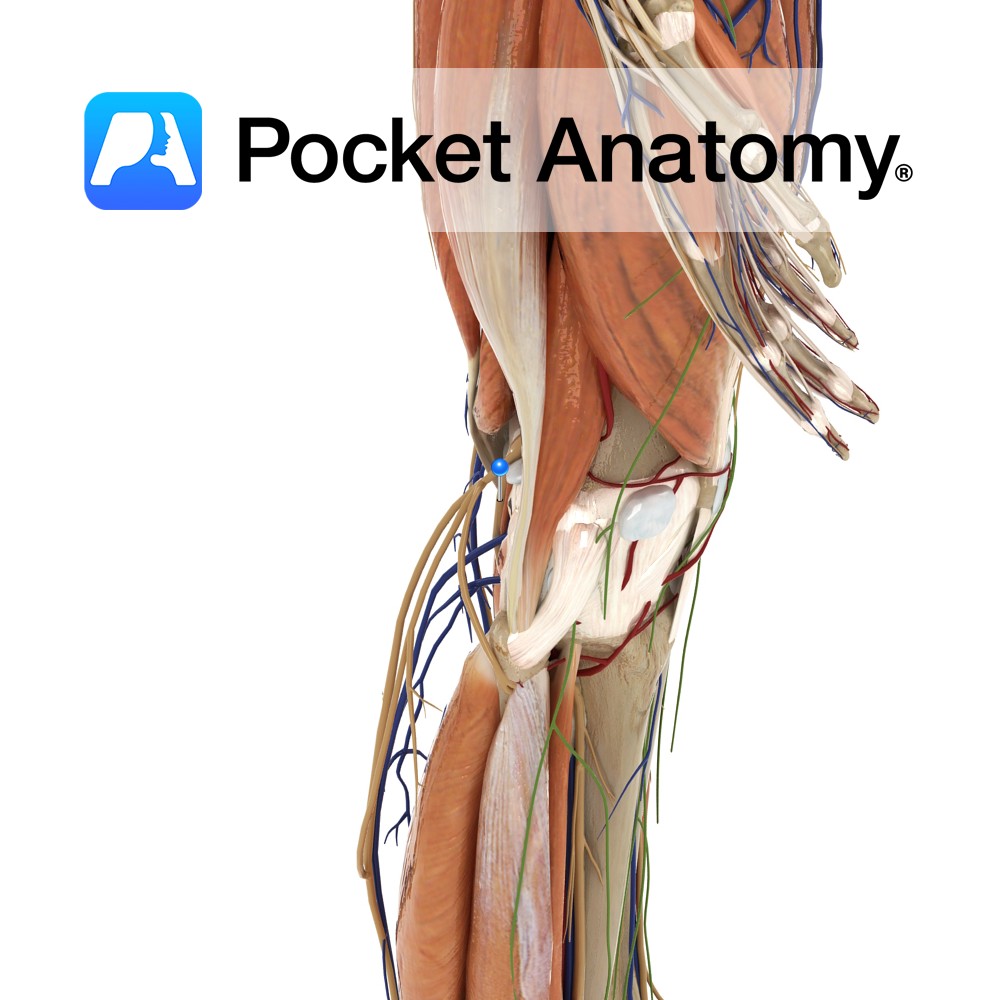
Anatomy Course A terminal branch of the sciatic nerve, and so contains fibres from the spinal segments of L4 – S3. The sciatic nerve becomes the tibial nerve upon exiting the popliteal fossa. It passes under the tendinous arch formed by the soleus muscle and descends in the plane between the solus and the tibialis
- Published in Pocket Anatomy Pins

Anatomy Large long bulge front of upper shaft, where patellar ligament (ie central part of common tendon of quadriceps femoris; rectus femoris, vastus medialis, intermedius and lateralis). Clinical The tuberosity has an apophysis and fractures can occur in active adolescents. Osgood-Schlatter disease/syndrome is an associated, usually self-limiting painful condition affecting active children 9-16 (boys 5:1
- Published in Pocket Anatomy Pins

Anatomy Prominent ridge/crest on upper part of back of tibia; insertion of politeus from above; origins of soleus, flexor digitorum longus, tibialis posterior to below. Interested in taking our award-winning Pocket Anatomy app for a test drive?
- Published in Pocket Anatomy Pins

Anatomy Prismoid, broader at top than bottom, a little narrower in middle, runs down vertically (unlike femur which runs down and in). Clinical Skin and cubcutaneous covering of anterior and medial aspects of tibia very thin, so many fractures are open (ie skin broken, with increased risk bone infection – osteomyelitis) whereas fibula well padded.
- Published in Pocket Anatomy Pins

Anatomy Strong prong projecting down from medial/outer side of lower extremity, articulating laterally with the talus. Clinical Fractures can be isolated or more often, one of; bi-malleolar (with lateral malleolus -often requires surgery; tri-malleolar with lateral malleolus and posterior aspect of bottom of tibia – usually requires surgery; fracture often accompanied by ligamentous damage. Vignette
- Published in Pocket Anatomy Pins

Anatomy Swelling on inside of upper extremity, to which MCL (tibial/medial collateral ligament, from medial epicondyle of femur above) is attached. Clinical Medial collateral ligament (MCL) injury common. MCL protects against varus angulation. Vignette Knee joint stability provided in part by shape of articular surfaces of femur and tibia, also by cruciate ligaments (anterior and
- Published in Pocket Anatomy Pins

Anatomy Swelling on outside of upper extremity, articulates with head of fibula, gives attachment to iliotibial band/tract. Clinical Knee joint allows flexion, extension and small amount lateral and medial rotation. Vignette Tibia is 2nd longest behind femur, and is the weightbearing bone of the leg. . Interested in taking our award-winning Pocket Anatomy app for
- Published in Pocket Anatomy Pins
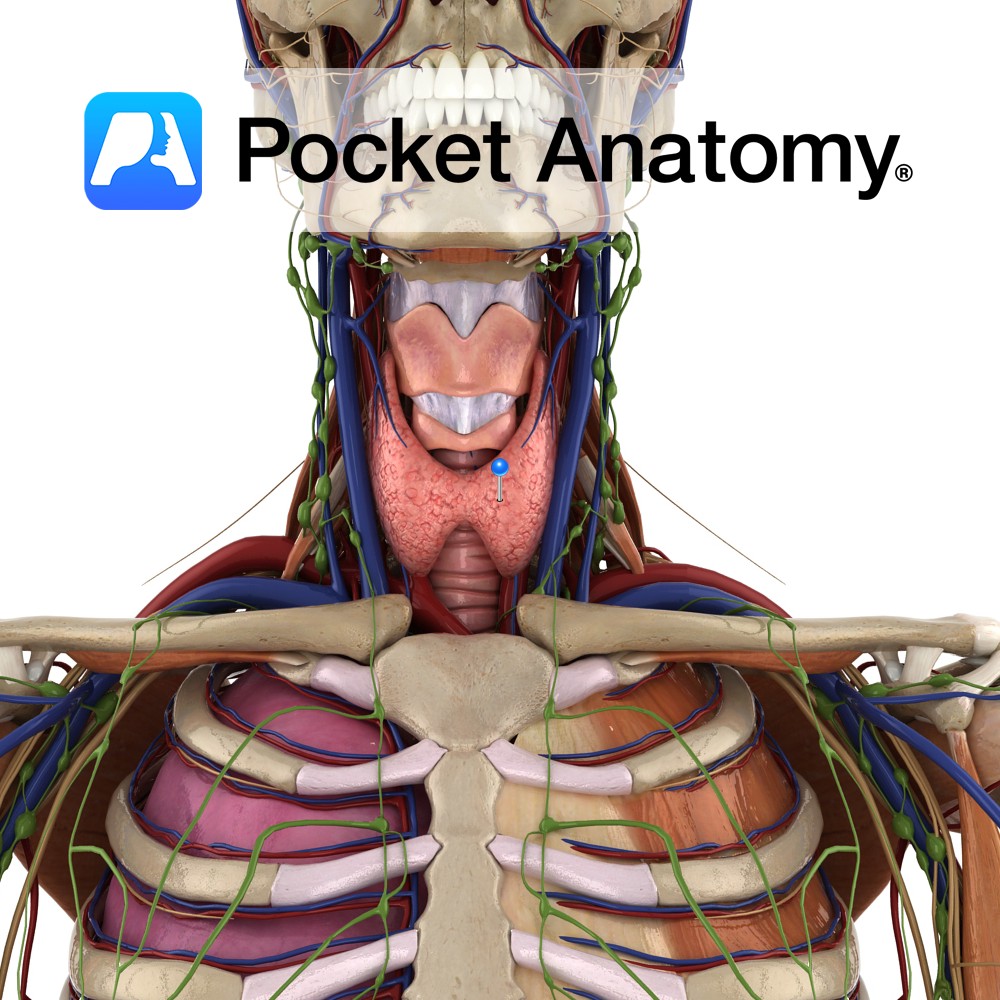
Anatomy Largest endocrine gland, in neck, ductless, butterfly-shaped (2 conical lobes, apex up, connected by isthmus), behind infrahyoid (strap) and sternocleidomastoid muscles, partially wrapping around posterior structures – thyroid and cricoid cartilages (attached to them, so moves on swallowing), trachea, esophagus. Encapsulated, between the 2 layers of which, posteriorly, are 2 parathyroid glands each side.
- Published in Pocket Anatomy Pins
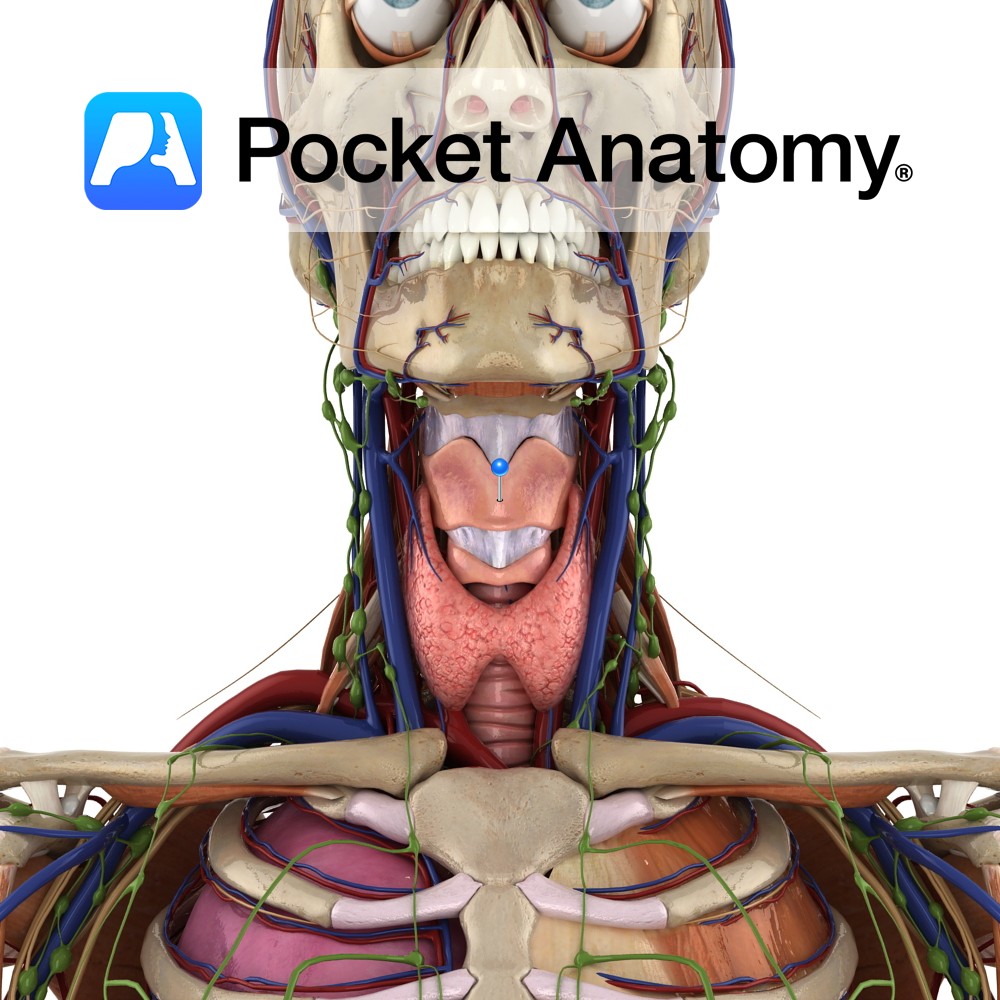
Anatomy The largest part of the larynx. It comprises of two quadrangular lamina, fused along the inferior two thirds to form the laryngeal prominence. The posterior border of each lamina projects as superior and inferior horns. The superior horns attaches to the hyoid bone via the thyrohyoid membrane. The inferior horns articulate with the cricoid
- Published in Pocket Anatomy Pins